The word “brief” makes some clinicians nervous. It sounds like a constraint imposed by insurance companies, managed care organizations, or tight-fisted institutional budgets. It sounds like a compromise.
It is not a compromise. Brief therapy is a clinical stance.
The Ten-Session Model
Haley’s approach to therapy was designed around a specific structural reality: most clients who will benefit from treatment can be helped within ten sessions. Some need fewer. A small number need more. But the ten-session framework is not an arbitrary limit. It reflects what happens clinically when the therapist focuses on the presenting problem and designs interventions to change the behavioral pattern that maintains it.
In the first session, the therapist defines the problem in behavioral terms, identifies the relational structure surrounding it, and assigns a directive. In subsequent sessions, the therapist evaluates the result of the directive, adjusts the intervention, and addresses new information as it emerges. Change is measured against the presenting complaint. When the client no longer has the problem they came in with, therapy ends.
This model produces results because it operates under pressure. A ten-session limit forces the therapist to be specific about the problem, efficient in assessment, and deliberate in intervention design. The therapist who knows they have ten sessions does not spend three sessions building rapport, two sessions collecting history, and two more sessions exploring the client’s childhood. The therapist gets to work.
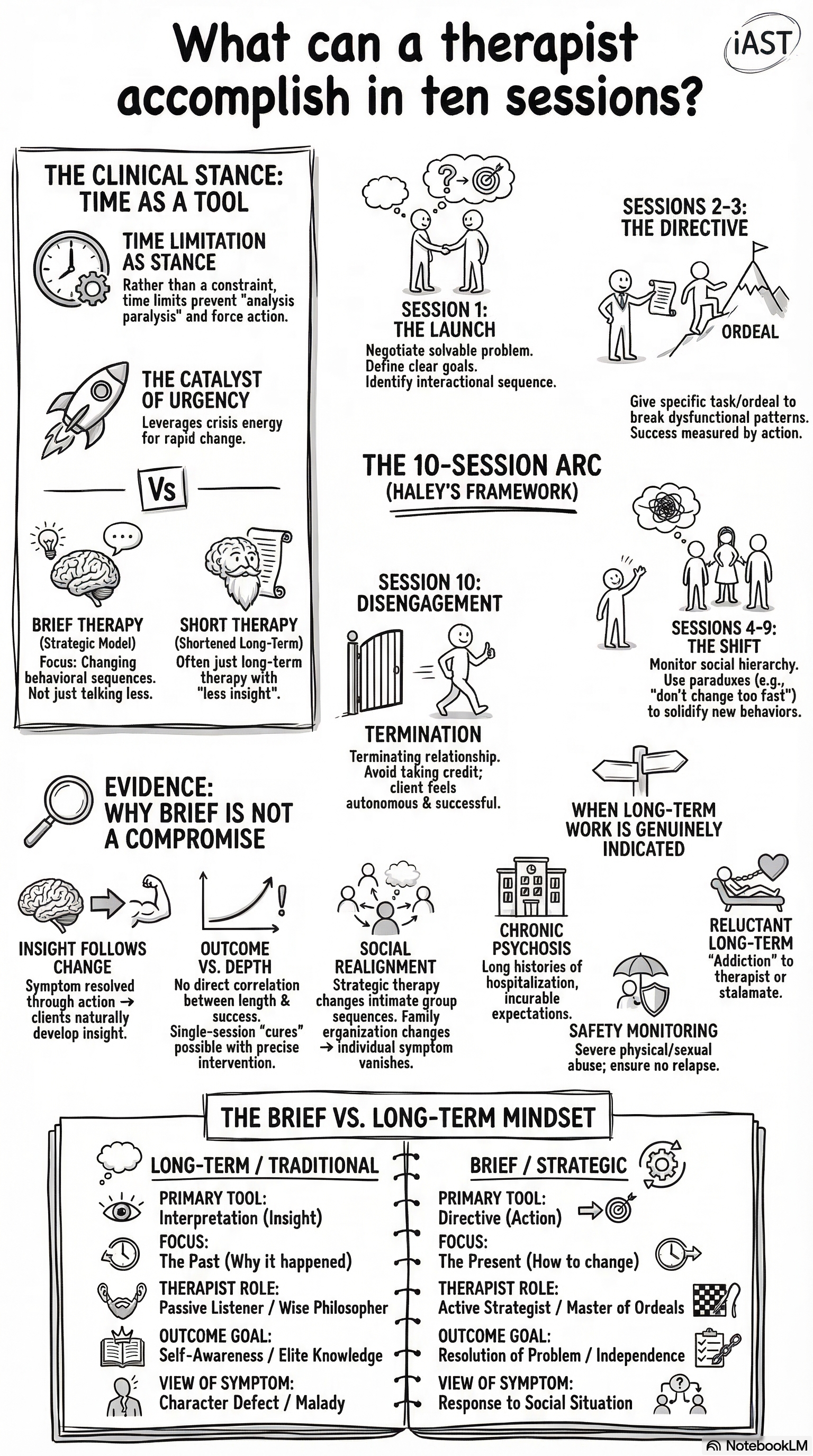
Brief Therapy vs. Short Therapy
There is a difference between therapy that is brief and therapy that is short. Short therapy is therapy that ends quickly, for any reason. The client drops out after two sessions. The insurance company authorizes six sessions and the therapist fits whatever they can into the time available. The clinician applies their usual approach in compressed form.
Brief therapy is designed from the ground up to produce change in a limited number of sessions. The assessment is focused on the presenting problem, not on comprehensive diagnostic formulation. The interventions are behavioral, not exploratory. The therapist takes an active role, assigning tasks and making clinical decisions, rather than following the client’s lead. The brevity is not a constraint on the method. The brevity is the method.
The question is not whether short-term work is effective. The question is whether the practitioner knows how to use the time.
Haley was direct about why brief therapy works: “If you are going to fail, you might as well fail quickly.” A long-term therapy that produces no change in the presenting problem after fifty sessions has wasted forty-nine sessions. A brief therapy that produces no change after ten sessions has wasted nine. The client is free to seek a different approach sooner. The cost in time, money, and suffering is lower.
The Evidence Base
Brief therapy has accumulated a substantial evidence base across multiple decades and clinical populations. The MRI group published outcome data showing that their brief therapy model resolved presenting problems in an average of seven sessions. Haley’s strategic approach produced comparable results with family systems and individual clients.
Contemporary research supports what these clinicians observed in practice: for the majority of presenting problems, including anxiety, depression, relationship conflict, and behavioral disorders in children, therapeutic gains plateau after six to ten sessions. Additional sessions produce diminishing returns. The bulk of change occurs early in treatment, when the therapeutic relationship is new and the client is most motivated to engage with novel interventions.
This does not mean that long-term therapy has no place. Some presentations benefit from extended treatment: complex trauma, personality disorders, chronic psychotic conditions. Strategic practitioners recognize these cases and adjust their approach accordingly. The ten-session model is a default, not a rule. The practitioner who starts with a brief orientation and extends treatment when clinically indicated makes better decisions than the practitioner who starts with an open-ended orientation and hopes that something useful happens eventually.
What the Strategic Practitioner Does Differently
Even when treating cases that require more than ten sessions, the strategic practitioner operates differently from the long-term therapist. Each session has a specific purpose. Each intervention is designed to produce a specific behavioral change. The therapist evaluates progress against the presenting complaint at every session and adjusts the strategy when progress stalls.
Long-term therapists often describe their work as “creating a space” for the client to grow. Strategic therapists create pressure. The directive introduces a new variable into the client’s behavioral system. The system responds. The therapist reads the response and designs the next intervention. The therapeutic process is iterative: act, observe, adjust. It does not require extensive processing time. It requires clinical precision.
This approach demands more of the therapist per session than most other modalities. The brief therapist cannot coast. Every session counts, and every session must move the case forward. The training implications are significant: a clinician who learns strategic therapy must develop the capacity to assess quickly, intervene decisively, and tolerate the anxiety of not knowing everything about the client before acting. These are skills that many training programs neglect, and they are the skills that brief therapy runs on.