A directive is a task the therapist assigns the client to perform between sessions. It is the primary instrument of change in strategic therapy. Where insight-based approaches wait for the client to understand their problem, the directive approach produces behavioral change first and lets understanding follow if it follows at all.
Jay Haley devoted an entire chapter of Problem-Solving Therapy to the art of giving directives, and for good reason. The directive is where strategic therapy happens. Everything else, the assessment, the reframing, the therapeutic relationship, serves the directive. If the client completes the task, the structure of the problem changes. If the client does not complete the task, the practitioner gains information about the pattern of resistance and adjusts.
What a Directive Is Not
A directive is not homework in the sense that CBT uses the term. CBT homework asks the client to practice a skill: record thoughts, challenge cognitive distortions, complete an exposure hierarchy. The goal is for the client to internalize a corrective process.
A strategic directive is different. It is designed to alter the relational structure of the problem. The client may not understand why the task works. The therapist may not explain why the task works. The task works because it changes the behavioral pattern that maintains the symptom.
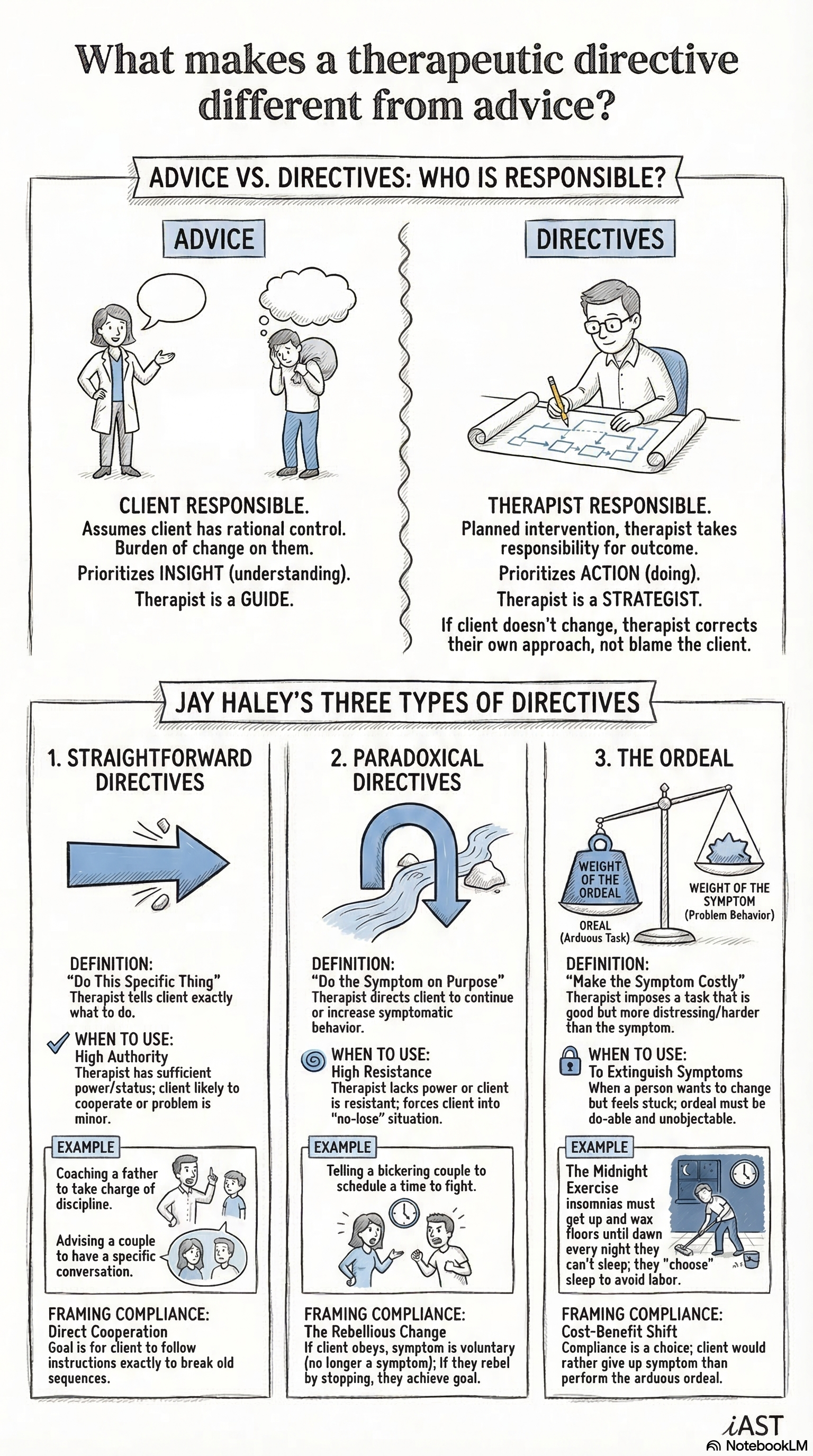
A directive is also not advice. Telling a depressed client to “get more exercise” is advice. Assigning a depressed client a specific behavioral task at a specific time, with specific instructions about who should know about it and who should not, is a directive. The specificity matters. The structure matters. The directive succeeds because it is designed for the particular relational dynamics of the particular case.
Three Formats
Haley described three primary formats for therapeutic directives.
Straightforward directives ask the client to do something the therapist believes will help. A couple who never talks assigns one partner to ask the other a specific question at a specific time each day. A parent whose child refuses to eat stops discussing food at mealtimes. The instruction is clear, the rationale is transparent, and the client complies because the task makes sense to them.
Straightforward directives work best with clients who are cooperative, who want to change, and who have the capacity to follow through. Many clients fit this description, and a straightforward directive is the most efficient intervention available.
Paradoxical directives ask the client to continue or intensify the symptom. A man who cannot sleep is instructed to stay awake all night. A woman who has panic attacks is told to schedule a panic attack at a specific time. The logic: if the therapist prescribes the symptom, the client’s involuntary behavior becomes a voluntary act. Voluntary symptoms are symptoms the client controls, and symptoms the client controls lose their power.
Paradoxical directives are appropriate for clients who resist straightforward intervention. The resistant client who refuses to follow instructions finds that refusing the paradoxical directive produces the therapeutic change the therapist intended.
Ordeal directives assign the client a task that is more unpleasant than the symptom. A client who wakes at three in the morning with anxiety is instructed to get out of bed at three and clean the house for two hours. The symptom becomes associated with an undesirable consequence. The client faces a simple calculation: keep the symptom and do the ordeal, or give up the symptom. Most clients give up the symptom.
The directive succeeds because it changes the behavioral pattern that maintains the symptom. Insight is optional.
Designing for Compliance
The art of giving directives is the art of designing for compliance. A directive that the client will not perform is a wasted intervention. Haley emphasized several principles for increasing the likelihood that the client completes the task.
The directive must be specific. “Communicate more” is vague. “Every evening at eight, ask your partner this question and listen for three minutes without responding” is specific. Vague directives fail because they give the client room to avoid the behavioral change.
The directive must be framed within the client’s motivational structure. A client who comes to therapy to save their marriage will complete a directive framed as necessary for the marriage. A client who comes because they are in pain will complete a directive framed as pain relief. The same behavioral task can serve different presentations depending on how the practitioner frames it.
The directive must account for the likely response of other people in the system. A wife who changes her behavior at home will get a reaction from her husband. If the therapist does not anticipate and prepare for that reaction, the directive may destabilize the system in ways that cause the client to abandon the task.
Why This Works Faster Than Insight
Insight-based therapy operates on a specific theory of change: if the client understands the origins and dynamics of their problem, the understanding itself will produce change. Decades of clinical evidence suggest that this theory is sometimes correct and often incomplete. Many clients understand their problems thoroughly and continue to have them.
Directive therapy operates on a different theory: if the client changes their behavior, the problem changes. This theory is faster because behavior is immediately modifiable. The client does not need to reconstruct their childhood, process their emotions, or develop a new self-narrative. The client needs to do the task. When the task alters the relational structure of the problem, the symptom loses its function and remits.