Jay Haley was not a psychiatrist, a psychoanalyst, or a clinical psychologist. He was a communications analyst who spent a decade on Gregory Bateson’s research project studying patterns of interaction in schizophrenic families, hypnotic inductions, and therapeutic encounters. That outsider position gave him something the clinical establishment lacked: the ability to describe what therapists actually do, rather than what they say they do.
The Bateson Years
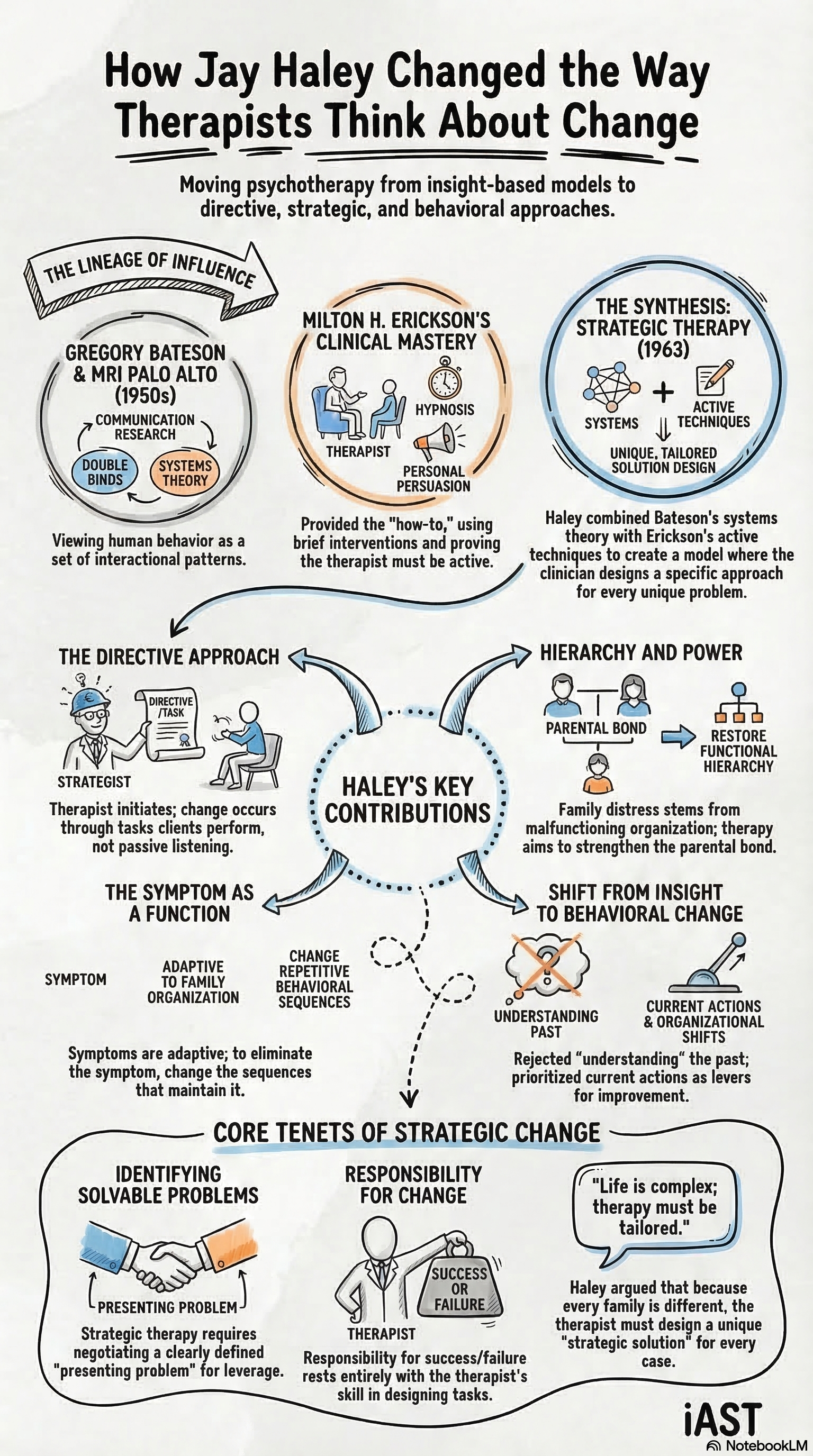
From 1952 to 1962, Haley worked as a full-time member of Bateson’s project at the Veterans Administration Hospital in Palo Alto. The group, which included John Weakland and consulting psychiatrists Don D. Jackson and William F. Fry, published over seventy articles and books on communication, paradox, and schizophrenia. Their central contribution was the double-bind theory: the observation that contradictory messages delivered within relationships of dependence produce the patterns clinicians label as mental illness.
Haley’s specific contribution was applying communication analysis to the therapy session itself. He watched what therapists did. He watched what hypnotists did. He noticed that the same interactional patterns appeared in both: the contest over who defines the relationship, the use of paradox to bypass resistance, the strategic deployment of ambiguity. These observations became the foundation of his clinical method.
Training Under Erickson
While working on the Bateson project, Haley began visiting Milton H. Erickson in Phoenix. Over the next seventeen years, he studied Erickson’s techniques in detail, eventually producing Uncommon Therapy (1973), the book that introduced Erickson’s clinical methods to a broad professional audience.
From Erickson, Haley learned the directive approach to therapy. Erickson did not wait for clients to achieve insight. He assigned tasks, told stories, prescribed behaviors, and used the client’s own resistance as material for intervention. Haley recognized that Erickson’s methods worked because they operated on the structure of the problem rather than on the client’s understanding of it. This principle became the core of strategic therapy.
Strategies of Psychotherapy
In 1963, Haley published Strategies of Psychotherapy, the book that defined the field. The table of contents reads like a blueprint for everything that followed: “Symptoms as Tactics in Human Relationships,” “Techniques of Directive Therapy,” “The Therapeutic Paradoxes.” The central argument was that all psychotherapy is strategic, whether the therapist admits it or not. Every therapeutic intervention positions the therapist in relation to the client. The question is whether the therapist does this deliberately or accidentally.
The book examined psychoanalysis, directive therapy, and hypnosis through the same communication lens. Haley showed that psychoanalysts who claimed to be neutral were, in fact, executing a specific relational strategy. The analyst’s silence, the refusal to answer questions, the insistence on free association: these are tactical moves. The difference between strategic therapy and other approaches is not that the strategic therapist manipulates and others do not. The difference is that the strategic therapist knows what they are doing.
The question is not whether the therapist manipulates. The question is whether the therapist does so with skill and awareness or by accident.
The Philadelphia Years and Beyond
In 1967, Haley moved to the Philadelphia Child Guidance Clinic, where he worked alongside Salvador Minuchin and Braulio Montalvo. This period produced Problem-Solving Therapy (1976), which shifted the unit of analysis from the dyad to the triad. Every clinical problem, Haley argued, involves at least three people. The symptom-bearer, the person most affected by the symptom, and a third party whose involvement maintains the pattern. Therapy that ignores the triangle misses the structure of the problem.
Haley later founded the Family Therapy Institute in Washington, D.C., with Cloe Madanes. There he published Leaving Home (1980), on the therapy of disturbed young people, and Ordeal Therapy (1984), which formalized the technique of assigning clients tasks more unpleasant than their symptoms. The ordeal principle is straightforward: if giving up the symptom becomes easier than keeping it, the client gives it up. The technique sounds crude until you watch it work with cases that have defeated every other approach.
Why Haley Still Matters
The field has moved through several fashions since Haley’s peak influence in the 1980s. Narrative therapy, solution-focused therapy, and the collaborative model all gained popularity by positioning themselves against the directive tradition. Michael P. Nichols, writing the foreword to The Art of Strategic Therapy in 2003, noted that “some people would say that strategic therapy is dead.” He then spent the next several pages explaining why those people were wrong.
Haley’s framework remains the sharpest instrument in brief therapy for a specific reason: it asks the right question. Where other approaches ask “What is wrong with this person?”, strategic therapy asks “What is this symptom doing, and for whom?” That question changes everything about how a practitioner designs an intervention. The method is economical, testable, and effective with the populations that other modalities struggle to reach.