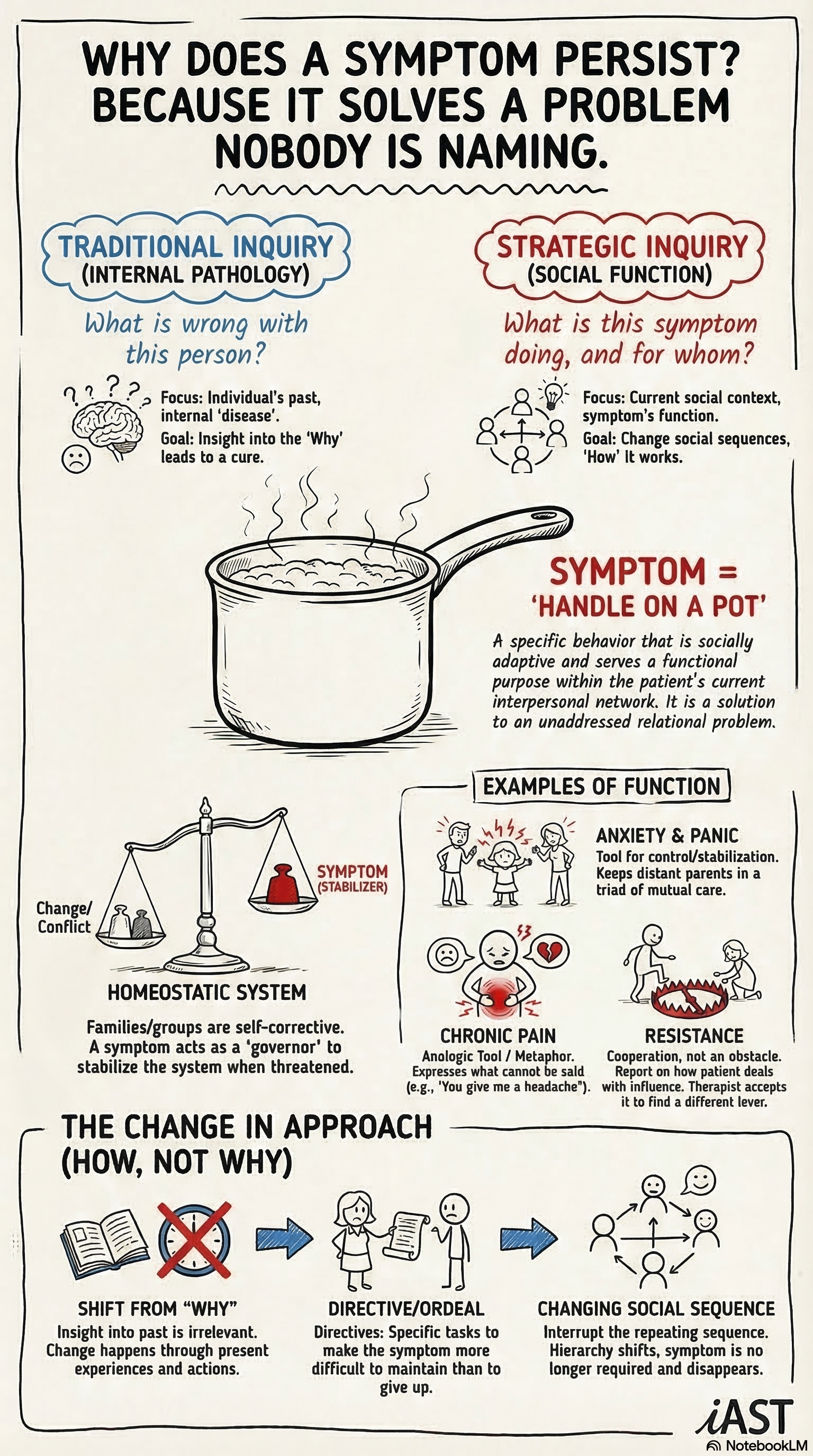
The reframe at the center of strategic therapy is this: a symptom is not a disease. It is a solution. The client developed the symptom because it serves a function within their relational system, and the symptom will persist as long as that function remains necessary.
This is not a metaphorical claim. It is a diagnostic framework that changes what a practitioner looks for and what a practitioner does.
The Clinical Logic
A woman presents with panic attacks that occur every evening when her husband arrives home from work. A linear diagnostic model treats the panic as a disorder: measure its severity, identify its triggers, prescribe medication or teach coping strategies. A strategic model asks a different question. What does the panic attack accomplish?
The panic attack reorganizes the evening routine. The husband, who otherwise disengages, must attend to his wife. The couple avoids the conflict they cannot resolve. The children are recruited into a caretaking role. The symptom structures the household’s relational patterns in a way that no one consciously designed but everyone participates in maintaining.
The strategic practitioner does not tell the client that her panic is “functional.” That framing belongs to the clinician’s analysis, not the client’s experience. The practitioner uses the analysis to design an intervention that addresses the relational structure. If the couple can address their conflict directly, the panic loses its function and remits.
How This Changes the Question
Most therapeutic models begin with some version of the question “What is wrong with this person?” The strategic model begins with “What is this symptom doing, and for whom?”
The second question is harder to answer. It requires the practitioner to see the presenting problem in its relational context: who else is affected, who benefits from the symptom’s presence, who would be destabilized by its absence. A child’s school refusal keeps a lonely parent company. An adult’s chronic pain excuses them from a career they cannot face. An adolescent’s substance use stabilizes a marriage by giving both parents a shared project.
A symptom is not a disease to be cured. It is a solution to a relational problem the client has not yet solved by other means.
None of this implies that the client is faking, malingering, or choosing to be symptomatic. The function operates below the level of conscious intention. The client’s suffering is genuine. The practitioner’s job is to understand what the suffering accomplishes within the system and then to make it unnecessary.
Applications Across Presentations
Anxiety. Anxiety disorders often serve a regulatory function in relationships. The anxious partner receives reassurance and attention. The non-anxious partner maintains a position of competence and control. Both partners participate in maintaining the pattern. Interventions that target only the anxious individual miss the relational structure that feeds the symptom.
Chronic pain. Pain without clear physiological cause is one of the most common functional symptoms in clinical practice. The pain restricts activity, elicits care, and communicates distress that the client cannot express verbally. Strategic approaches to psychosomatic pain focus on the communicative and relational functions of the pain, not on the pain itself.
Resistance. A client who resists treatment is demonstrating a functional behavior. The resistance protects something: autonomy, a relationship, a self-concept, a secondary gain from the symptom. Strategic therapy does not fight resistance. It reads resistance as information about what the symptom is protecting and designs interventions accordingly.
The Practical Implication
Reading symptoms as functions is not a theoretical exercise. It is a clinical skill that changes the practitioner’s behavior in session. A practitioner who understands functional analysis asks different questions in the first interview. “Who else is affected by this problem? What happens in the household when the symptom is present? What would change if the symptom disappeared tomorrow?” These questions generate the information needed to design an effective intervention.
The skill takes practice. Most clinicians are trained to think in terms of diagnosis and treatment: identify the disorder, apply the protocol. Strategic therapy asks the practitioner to think in terms of patterns and structures: identify the function, alter the structure. The shift is significant, and it produces results with populations that diagnostic-driven approaches often fail to reach.