Milton Erickson operated from a principle that most clinical traditions ignore: everything the client brings into the session is usable. The symptoms, the resistance, the personality quirks, the metaphors they speak in, the way they sit in the chair. None of it is an obstacle. All of it is material.
This principle, which Erickson called utilization, is the foundation of his clinical method and one of the core concepts of strategic therapy.
What Utilization Means in Practice
A client who speaks only in abstractions receives an intervention delivered in abstractions. A client who is concrete and literal receives concrete, literal instructions. A client who resists every suggestion is given a suggestion designed so that resistance to it produces the desired outcome. A client who is obsessively punctual is assigned a task that uses punctuality as the mechanism of change.
The practitioner does not try to change the client’s style, personality, or preferred mode of engagement. The practitioner works with what is there. The clinical question is not “How do I get this client to cooperate?” The clinical question is “How do I build an intervention using the materials this client has already provided?”
Erickson demonstrated this principle across thousands of cases. A man who was obsessively rigid received a directive that required rigid adherence to a new behavioral routine, one that happened to resolve his presenting complaint. A woman who insisted on controlling every aspect of the therapy was given a therapeutic task that required her to exercise even more control, directed at the structure of her problem. The intervention succeeded because it used the client’s own behavioral tendencies as the engine of change.
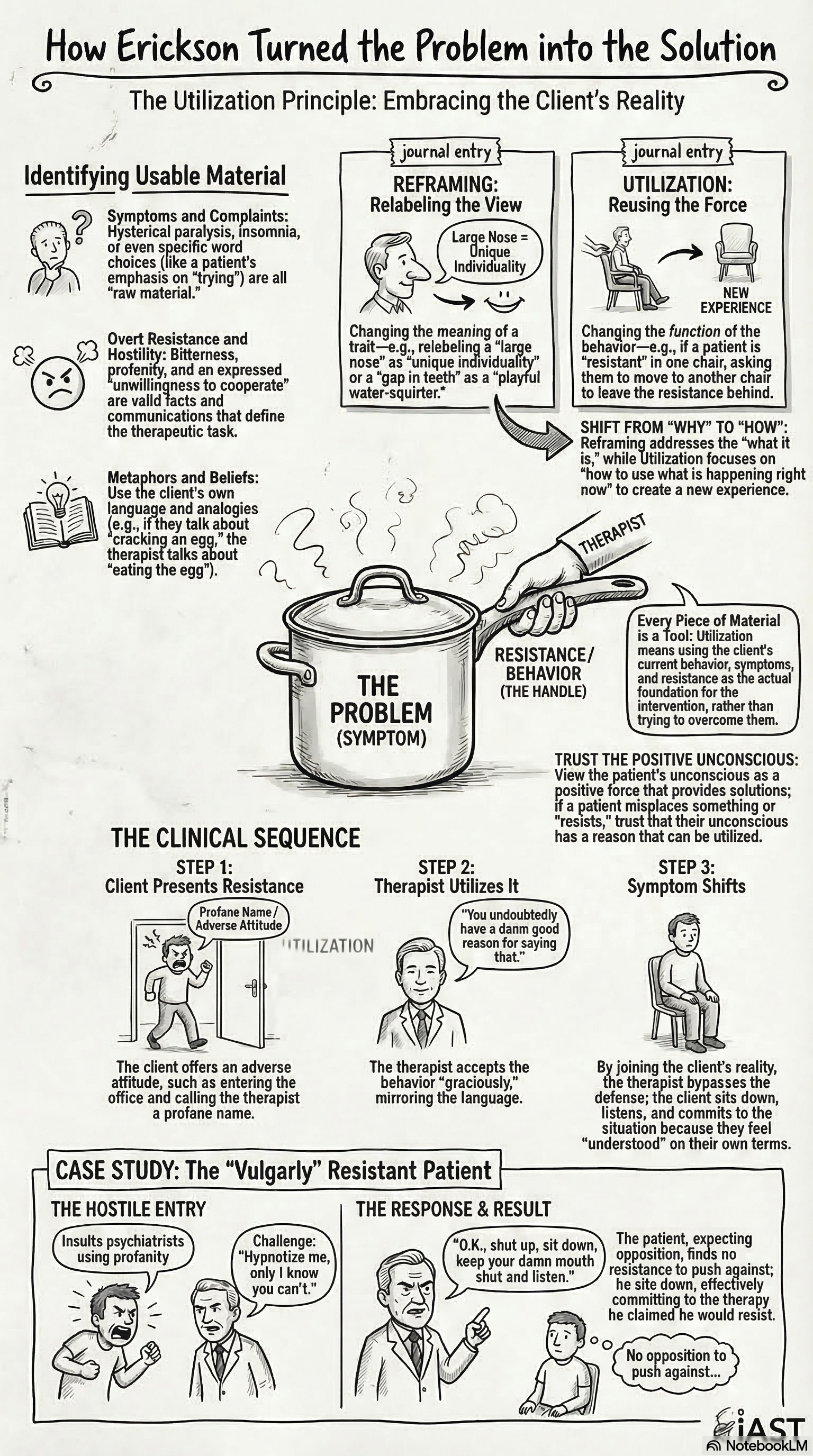
The Difference Between Utilization and Reframing
Reframing tells the client that their problem means something different than they thought. “Your anxiety is actually your body trying to protect you.” The client receives a new cognitive frame and may or may not find it useful.
Utilization does not reinterpret the problem. It uses the problem. The anxious client’s anxiety is not reframed as protection. The anxious client’s pattern of hypervigilance is directed toward a task that produces therapeutic change. The client does not need to adopt a new interpretation. The client needs to do what they are already doing, pointed in a different direction.
Utilization does not reinterpret the problem. It uses the problem. The client's own patterns become the mechanism of change.
This distinction matters clinically. Reframing works with clients who are interested in understanding themselves. Utilization works with everyone, because it does not require the client to adopt a new perspective. It requires only that the client continue being who they already are.
Identifying Usable Material
The practitioner trained in utilization listens differently in session. The standard clinical interview collects information about the problem: onset, duration, severity, previous treatment. The utilization-oriented interview also collects information about the client’s resources: behavioral tendencies, relational patterns, areas of competence, sources of motivation.
Some questions that orient toward utilization:
What does the client do well? A client who is organized and disciplined can be given structured directives that use their organizational skills. A client who is spontaneous and impulsive may respond better to directives that use improvisation.
What is the client’s pattern of resistance? A client who argues with every suggestion is demonstrating a strong oppositional tendency. That tendency is usable. Prescribe the opposite of what you want, and the client’s opposition produces the desired result.
What metaphors does the client use? A client who describes their depression as “being in a hole” has given the practitioner a ready-made metaphor. Directives can be framed using the client’s own language: tasks that involve “climbing,” “reaching,” or “stepping up.” The metaphor does the framing work that the therapist would otherwise have to construct from scratch.
What is the client’s relationship to the symptom? Some clients hate their symptoms and want them gone immediately. Others are ambivalent. A client who is ambivalent about change is providing information: the symptom serves a function they are not ready to give up. The practitioner who recognizes this ambivalence can design an intervention that addresses the function without requiring the client to commit to full change immediately.
Utilization in the Strategic Framework
Within Haley’s strategic therapy, utilization operates as a design principle for directives. The directive should use whatever the client brings: their compliance, their resistance, their behavioral patterns, their relational dynamics. A well-designed directive fits the client the way a key fits a lock. It works because it is built from the client’s own materials.
This is what separates strategic therapy from manualized approaches. A manualized protocol applies the same intervention to every client with the same diagnosis. A strategic intervention is constructed for the specific client sitting in the specific chair at the specific moment. The diagnosis is less important than the pattern. The protocol is less important than the fit.
Practitioners who develop the skill of utilization find that they have more options with difficult cases. The client who defeats every standard intervention has given the practitioner an enormous amount of information about what does not work. The practitioner who can use that information, who can build the next intervention from the wreckage of the previous ones, is practicing utilization.