Acceptance and Commitment Therapy arrived in the early 2000s as a “third wave” alternative to classical CBT. It challenged the cognitive model’s emphasis on correcting distorted thoughts and proposed instead that clients learn to accept their internal experiences while committing to value-driven behavior. Practitioners trained in ACT will find some of its principles familiar when they encounter strategic therapy, and some of its assumptions reversed.
Where the Two Converge
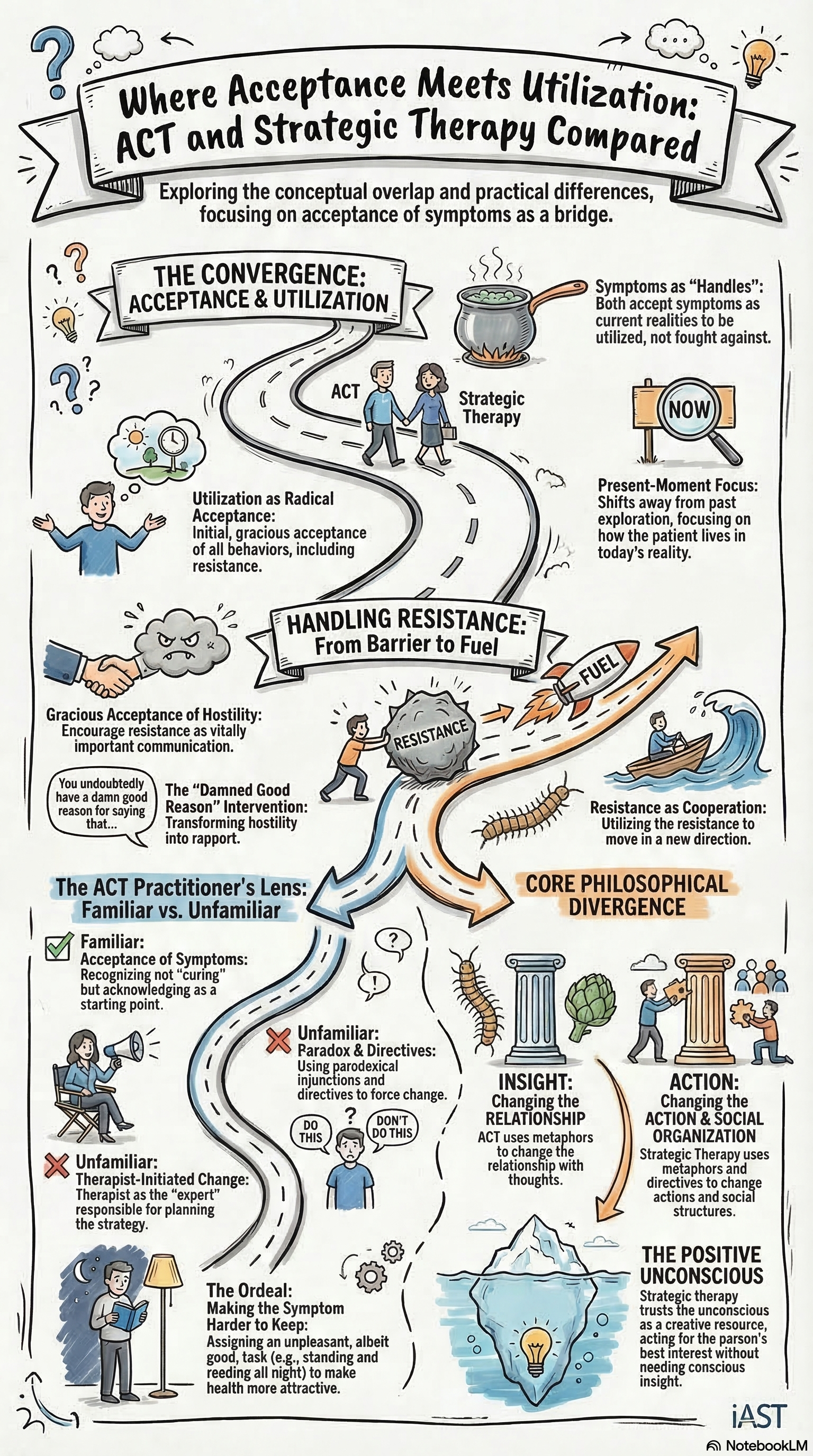
ACT and strategic therapy share a rejection of the premise that symptoms must be eliminated before the client can function. ACT teaches clients to accept difficult thoughts and feelings rather than fighting them. Strategic therapy, through the utilization principle, treats symptoms as material to be used rather than obstacles to be removed. Both approaches start from the position that the client’s experience is not the enemy.
The convergence goes deeper. ACT’s concept of “creative hopelessness,” the therapeutic move of helping the client recognize that their attempts to control internal experience have failed, resembles the strategic analysis of attempted solutions. The MRI model demonstrated that problems persist because of the solutions people apply to them. ACT demonstrates that psychological suffering persists because of the control strategies people apply to their thoughts and feelings. The structural analysis is similar: the solution is the problem.
Both approaches also prioritize behavioral change over cognitive insight. ACT asks clients to commit to value-driven actions regardless of how they feel. Strategic therapy assigns directives designed to alter behavioral patterns regardless of what the client understands about their situation. The emphasis on doing rather than understanding is shared ground.
Both ACT and strategic therapy treat the client's experience as material to work with, not an enemy to defeat.
Where They Diverge
The differences are significant and affect how each approach handles the clinical encounter.
The role of the therapist. ACT positions the therapist as a guide who helps the client clarify their values and commit to behavioral change. The process is collaborative: therapist and client work together to identify what matters and build a plan for action. Strategic therapy positions the therapist as a designer of interventions. The therapist assesses the relational structure of the problem and assigns directives to alter it. The process is directive: the therapist takes responsibility for the strategy.
This difference matters with resistant clients. ACT’s collaborative stance requires the client to engage in a reflective process. A client who will not engage, who dismisses values-based exploration, or who agrees in session and does nothing between sessions presents a challenge that ACT handles through motivational work. Strategic therapy handles the same challenge through paradoxical intervention, utilizing the resistance itself as the mechanism of change.
The unit of analysis. ACT works primarily at the individual level. The client’s relationship with their own thoughts and feelings is the therapeutic target. Strategic therapy works at the relational level. The client’s relationship with other people in their system is the therapeutic target. For individual presentations like anxiety or depression, both approaches can be effective. For relational presentations, family conflict, marital distress, or symptoms that serve a function within a system, the strategic framework provides tools that ACT’s individual orientation does not.
The handling of avoidance. ACT identifies experiential avoidance, the tendency to avoid unpleasant internal states, as the core pathological process. The therapeutic goal is to increase psychological flexibility so the client can experience discomfort without being controlled by it. Strategic therapy does not frame avoidance as pathological. If a client avoids something, the strategic practitioner asks what function the avoidance serves and designs an intervention around that function. The avoidance may be usable material, not a problem to be solved.
What the ACT Practitioner Finds Familiar
A practitioner trained in ACT who encounters strategic therapy will recognize several familiar elements. The emphasis on behavior over cognition. The acceptance of the client’s current state as the starting point. The skepticism toward interventions that depend on the client achieving insight.
The unfamiliar elements will be the directive stance, the relational analysis, and the use of paradox. ACT does not prescribe symptoms. ACT does not assign ordeals. ACT does not analyze the hierarchical structure of families. These tools expand the ACT practitioner’s repertoire for cases where the collaborative, values-based approach stalls.
Complementary, Not Competing
The most useful way to understand the relationship between these approaches is that they address different aspects of the clinical picture. ACT provides a framework for the client’s internal experience: how to relate to thoughts, feelings, and sensations without being controlled by them. Strategic therapy provides a framework for the client’s external situation: how the symptom functions within relationships and how to alter the relational structure that maintains it.
A practitioner who understands both approaches can read a case from the inside and the outside. When the presenting problem is primarily internal, ACT’s framework may be sufficient. When the presenting problem is embedded in a relational system, the strategic framework adds precision that ACT alone cannot provide. The two approaches do not cancel each other out. They illuminate different dimensions of the same clinical reality.