Cognitive Behavioral Therapy is the most widely taught, most heavily researched, and most broadly endorsed therapeutic approach in the English-speaking world. It works. For many presentations, it works well. The comparison here is not an argument against CBT. It is a clinical analysis of where the two approaches diverge and where a practitioner benefits from understanding both.
The Cognitive Model vs. the Relational Model
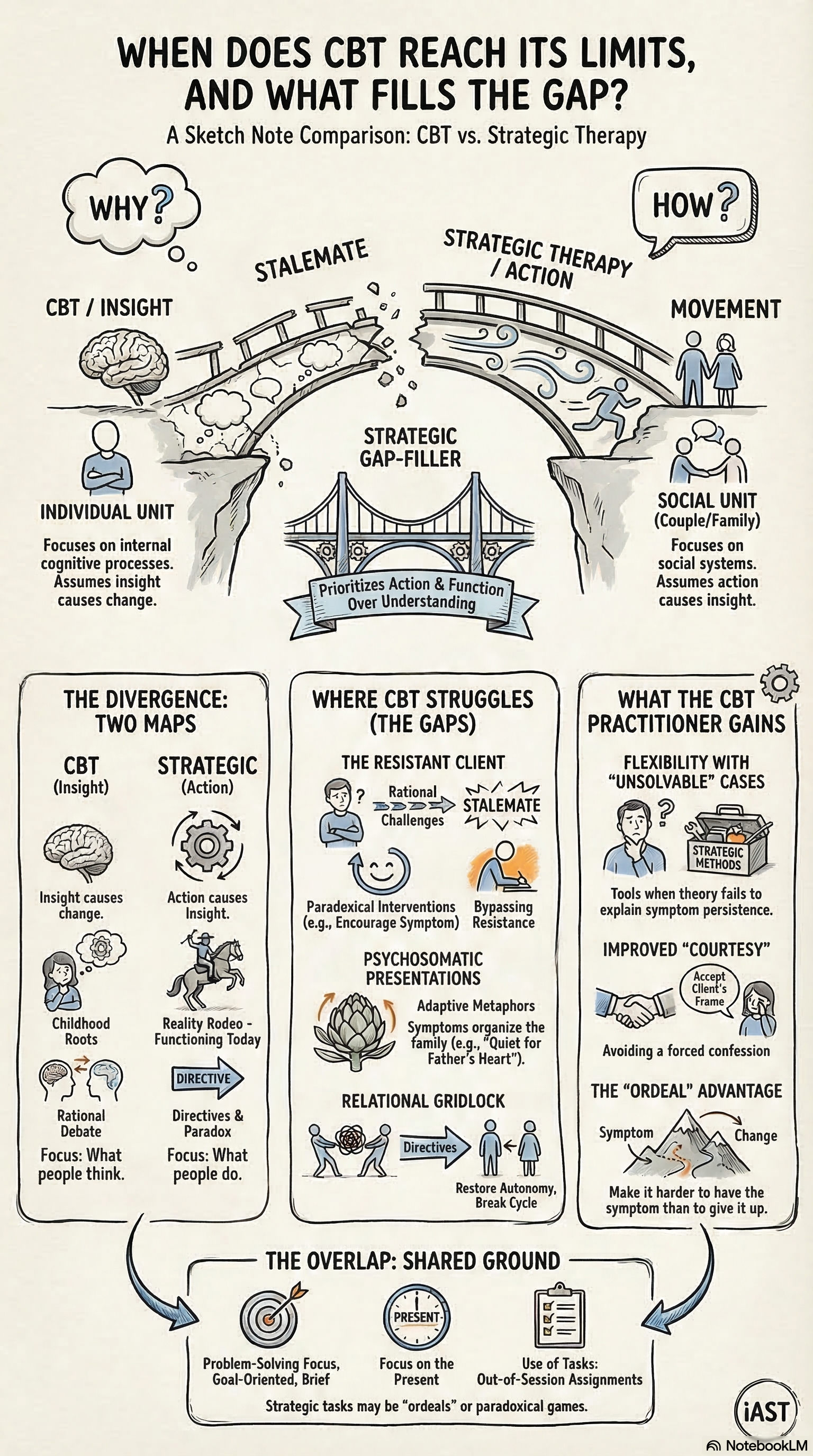
CBT operates on a cognitive model of symptoms. Anxiety results from distorted thinking. Depression results from negative automatic thoughts. The therapeutic intervention targets the cognition: identify the distortion, challenge it, replace it with a more accurate thought. Behavioral activation and exposure tasks reinforce the cognitive correction.
Strategic therapy operates on a relational model. Anxiety results from a behavioral pattern within a relational system. The therapeutic intervention targets the structure of the pattern: who does what, when, and what function the symptom serves. The practitioner assigns directives that alter the relational dynamics, and the symptom remits because its structural basis has changed.
Both models produce change. They produce change through different mechanisms, and they reach different populations.
Where CBT Excels
CBT is effective for presentations where the cognitive model fits. Generalized anxiety, mild to moderate depression, specific phobias, and performance anxiety respond well to cognitive restructuring and behavioral activation. The evidence base is strong because these presentations lend themselves to manualized protocols, controlled trials, and standardized outcome measures.
CBT is also excellent for psychoeducation. Clients who want to understand their symptoms, who are motivated to learn new skills, and who will complete homework between sessions thrive in CBT. The structured format gives clients a framework for understanding their experience and a set of tools they can continue to use after therapy ends.
CBT works best with clients who cooperate. Strategic therapy was designed for clients who do not.
Where CBT Reaches Its Limits
CBT struggles with three populations that strategic therapy handles well.
Resistant clients. CBT depends on client cooperation. The client must identify thoughts, challenge them in writing, complete exposure tasks, and practice new behaviors between sessions. Clients who will not do the homework, who argue with the cognitive model, or who agree in session and then ignore everything at home present a structural problem for CBT. The method has no mechanism for working with noncompliance other than motivational interviewing, which itself requires the client to cooperate with a conversational process.
Strategic therapy was built for noncompliance. The paradoxical directive uses resistance as the mechanism of change. The ordeal directive makes the symptom more costly than the intervention. The utilization principle turns the client’s behavioral tendencies into therapeutic resources. The client does not need to cooperate with the model. The model uses whatever the client does.
Psychosomatic presentations. Chronic pain without clear physiological cause, conversion symptoms, and functional neurological disorders are poorly served by cognitive restructuring. Telling a person with chronic back pain that their pain results from catastrophic thinking is both clinically inaccurate and relationally harmful. The pain is real. The cognitive model’s attempt to locate the problem in the client’s thinking misses the systemic function of the symptom.
Strategic therapy reads psychosomatic symptoms as functional behaviors within a relational system. The practitioner addresses the function rather than the cognition. This approach produces results with chronic pain populations that CBT protocols typically do not reach.
Relational problems. CBT was designed for individual symptom reduction. When the problem is a marriage, a family system, or a hierarchy that has broken down, the individual cognitive model cannot address the structural dynamics that maintain the symptoms. CBT for couples exists, but it grafts a relational orientation onto a framework that was designed for individual cognition. The fit is imperfect.
Strategic therapy treats the relational system as the primary unit of analysis. The intervention is designed for the system, not for the individual. For couples, families, and relational presentations, this framework is more precise.
What the CBT Practitioner Gains
A practitioner trained in CBT who adds strategic methods gains access to clients they currently cannot reach. The resistant client, the psychosomatic client, and the client embedded in a relational system all become workable when the practitioner can read behavioral patterns, design directives, and use resistance as material rather than treating it as an obstacle.
The addition does not require abandoning CBT. Many practitioners use CBT as their primary approach and deploy strategic techniques when the cognitive model stalls. The skill set is complementary. CBT provides structured protocols for straightforward presentations. Strategic therapy provides flexible, case-specific interventions for everything else.